Use 'Print preview' to check the number of pages and printer settings.
Print functionality varies between browsers.
Printable page generated Tuesday, 8 April 2025, 1:58 PM
Antenatal Care Module: 4. Hormonal Regulation of the Female Reproductive System
Study Session 4 Hormonal Regulation of the Female Reproductive System
Introduction
In the previous study session you learned about the anatomy and physiology of the female reproductive system. The hormones oestrogen and progesterone were briefly introduced. In this study session you will learn much more about the role of these and other important hormones involved in the regulation of the human menstrual cycle, the monthly production of mature ova (eggs) by females of reproductive age, and the preparation of the uterus as a welcoming environment for the start of a pregnancy.
Learning Outcomes for Study Session 4
When you have studied this session, you should be able to:
4.1 Define and use correctly all of the key words printed in bold. (SAQ 4.1)
4.2 Describe the physiological processes and changes during the menstrual cycle. (SAQs 4.1 and 4.2)
4.3 Describe the hormonal regulation of the female reproductive system. (SAQs 4.3 and 4.4)
4.1 The female reproductive hormones
As you will probably remember from your previous high school biology course, the various functions of the body are regulated by the nervous system and the hormonal system. Both these systems are involved in controlling the activity of the female reproductive system in a regular monthly series of events known as the menstrual cycle, as we will now describe.
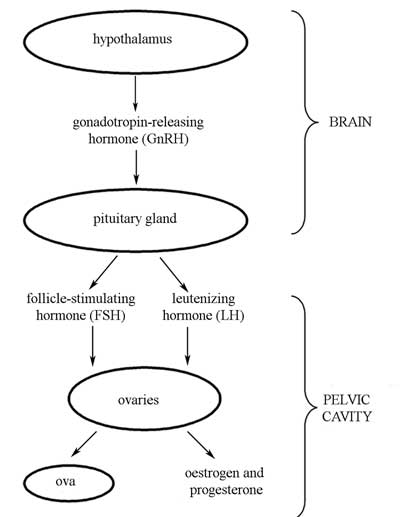
You should remember from Study Session 3 that a hormone is a signalling chemical produced in the body, which circulates in the blood; different hormones control or regulate the activity of different cells or organs. The functions of the five main hormones that regulate the female reproductive system are described in Box 4.1, and their interactions are illustrated in Figure 4.1.
Box 4.1 Hormones regulating the female reproductive system
Gonadotropin-releasing hormone (GnRH) is produced by a part of the brain called the hypothalamus. When it circulates in the blood, it causes the release of two important hormones (see below, and Figure 4.1) from the pituitary gland in another specialised part of the brain.
Gonadotropin is pronounced ‘gonn add oh troh pinn’. Hypothalamus is pronounced ‘hy poh thah lah mooss’. Pituitary is pronounced ‘pitt yoo itt ary’.
Follicle-stimulating hormone (FSH) is produced by the pituitary gland during the first half of the menstrual cycle. It stimulates development of the maturing ovarian follicle and controls ovum production in the female, and sperm production in the male.
Leutenizing hormone (LH) is also produced by the pituitary gland in the brain. It stimulates the ovaries to produce oestrogen and progesterone. It triggers ovulation (the release of a mature ovum from the ovary), and it promotes the development of the corpus luteum.
What is the corpus luteum? (Think back to Study Session 3.)
The name means ‘yellow body’, and after ovulation it develops in the ovary from the enlarged ovarian follicle that released the ovum.
Oestrogen is a female reproductive hormone, produced primarily by the ovaries in the non-pregnant woman. It promotes the maturation and release of an ovum in every menstrual cycle. It is also produced by the placenta during pregnancy.
Progesterone is produced by the corpus luteum in the ovary; its function is to prepare the endometrium (lining of the uterus) for the reception and development of the fertilised ovum. It also suppresses the production of oestrogen after ovulation has occurred.
The length of the menstrual cycle is typically 28 days, but it can be highly variable. In some women it may be as short as 21 days or as long as 39 days. The menstrual cycle is best understood if we focus first on events occurring in the ovaries, and then on events occurring in the uterus. We are going to describe each of them in turn.
4.2 The ovarian cycle
The ovarian cycle refers to the monthly series of events in the ovaries, associated with the maturation and release of an ovum, and the ‘just in case’ preparation for its fertilisation and implantation in the uterus. You may be wondering why the regulation of the female reproductive system is so complicated, as shown in Figure 4.1. The reason is that the ovarian cycle has to be initiated (switched on) and then suppressed (switched off) in a precisely regulated sequence every month. In this section, we will explain how this is achieved.
The ovarian cycle consists of two consecutive phases, each of about 14 days’ duration. Events are measured from ‘day 1’, which is the first day of the last normal menstrual period (LNMP).
4.2.1 The follicular phase: days 1 to 14
The sequence shown in Figure 4.1 begins with the secretion of GnRH from the hypothalamus, which stimulates the pituitary gland to produce FSH and LH, which in turn act on the ovaries, telling the ovarian follicles to complete the maturation of an ovum. During this period, a few ovarian follicles containing immature ova develop and mature under the stimulation of FSH and LH. Usually by day 14, only one follicle has become fully mature, and the ovum it contains is ready to be released. All other follicles that had begun maturing during this phase of the ovarian cycle degenerate as soon as ovulation has occurred.
Note that only one time interval is fairly constant in all females — the time from ovulation to the beginning of menstruation, which is almost always 14 to15 days. However, the time of ovulation is variable and difficult to predict accurately.
4.2.2 The luteal phase: days 15 to 28
This phase is the period of corpus luteum activity, during which the uterus is prepared ‘just in case’ of pregnancy. After ovulation has occurred, the corpus luteum begins to secrete progesterone, as well as a small amount of oestrogen. Progesterone maintains the uterus in a state ready to receive and nourish an embryo. The lining of the uterus (the endometrium) becomes thicker, more richly nourished by blood vessels, and more receptive to the fertilised ovum. Progesterone also inhibits any further release of FSH or LH from the pituitary gland.
Thus, ovulation is quickly followed by a rise in the level of progesterone in the circulation, as the corpus luteum takes over the production of this hormone. As the progesterone level rises, it circulates around the body in the blood. When a high concentration of progesterone reaches the hypothalamus in the brain, the effect is to stop the hypothalamus from producing GnRH.
What will happen when the hypothalamus stops producing GnRH? (Look back at Figure 4.1.)
The pituitary gland will stop producing FSH and LH.
What effect will this have on the ovaries?
The maturation of more ova will stop at that point.
This type of control system, where the rise in one body chemical (in this case, progesterone) stops the production of another body chemical (in this case, GnRH), is called a negative feedback mechanism. But the corpus luteum has a limited lifespan, and after it stops producing progesterone, the negative feedback on the hypothalamus stops, and this allows it to begin producing GnRH again. So the ovarian cycle begins all over again.
4.3 The uterine cycle
Next, we turn our attention to the events occurring in the uterus during the same (typically) 28-day period as the events just described in the ovaries. The uterine cycle indicates the cyclical changes that occur in the uterus in response to the female sex hormones, progesterone and oestrogen.
4.3.1 The menstrual phase: days 1 to 5
If fertilisation does not occur after ovulation, the corpus luteum will degenerate and production of progesterone will decrease, so the stimulus for maintaining the thick endometrium will disappear. The reduction in progesterone causes the shedding of the thick endometrial lining. The muscular wall of the uterus (the myometrium) contracts to help cut off the blood supply to the endometrium, causing it to break away from the uterus. The endometrium was richly supplied with blood vessels to nourish the fetus if a pregnancy occurred, so when it disintegrates and passes down the vagina, some blood is mixed in with it. The mixture of tissue and blood passes out through the vagina as the menstrual fluid (or menstrual flow), usually for a period of about three to five days. Other common names for menstruation are ‘monthly bleeding’ or ‘menstrual period’.
Menstruation usually occurs at monthly intervals throughout the reproductive years, except during pregnancy when it is completely suppressed and the woman cannot get pregnant again until after the baby is born. Breastfeeding a baby also suppresses menstruation, but there is a risk that ovulation and pregnancy may still occur.
4.3.2 The proliferative phase: days 6 to 14
The concentration of oestrogen in the blood is rising during this period, following the end of menstruation, as the ovaries prepare for the next ovulation at around day 14. It is called the proliferative phase (‘proliferate’ means to ‘multiply or increase’), because in this period the endometrium grows thicker and becomes more richly fed by blood vessels in preparation for the possibility of fertilisation and pregnancy.
4.3.3 The secretory phase: days 15 to 28
During this phase, the blood concentration of progesterone increases, which causes even more blood vessels to grow into the endometrium. This makes the endometrium receptive to the fertilised ovum. If the ovum is fertilised and the embryo implants in the endometrium and a placenta develops, it produces a hormone called human chorionic gonadotropin (HCG) throughout pregnancy. The detection of HCG in a woman’s urine is the basis of most pregnancy tests.
Chorionic is pronounced ‘korr ee onn ik’. Gonadotropin is pronounced ‘gonn add oh troh pinn’.
HCG signals the corpus luteum to continue to supply progesterone to maintain the thick, nourishing endometrium throughout the pregnancy. Continuous levels of progesterone act as a negative feedback mechanism on the hypothalamus and pituitary gland, preventing the release of FSH and LH, and hence further ovulation ceases.
What happens if fertilisation of the ovum does not occur?
The corpus luteum degenerates and the level of progesterone declines; the endometrium disintegrates and the woman menstruates — a signal that she did not become pregnant during that menstrual cycle.
4.4 The menarche, puberty and the menopause
You probably know that menarche (the first menstruation) starts on average between the ages of 12 to15 years in Ethiopia. But in some cases it can start as late as 17 to 20 years, or as early as 8 to 9 years. Some of the factors that affect the age of menarche are biological, and some are cultural.
Menarche is pronounced ‘menn ark’.
Menarche begins when the hypothalamus in the brain is sensitised to begin producing GnRH at around the age of 12 to15 years. But evidence suggests that GnRH may begin at an earlier age in girls who are well nourished and exposed to sexual motivating factors, such as watching sexual films and talking about sex. In malnourished girls, who have little exposure to sexual motivating factors, menarche may be delayed until the age of 17 to 20 years. Disease conditions that affect the hypothalamus and pituitary gland, or the ovaries and uterus, can also affect the age of first menarche.
Around the age of the menarche, the female sex hormones, oestrogen and progesterone, are responsible for the development of secondary sexual characteristics in the female. These include:
- the development of the breasts
- the broadening of the pelvis
- increased activity of sweat glands and sebaceous glands (oil glands in the skin)
- the growth of pubic and armpit hair.
Together with the menarche, the appearance of the secondary sexual characteristics marks the period known as puberty — the period of life (typically between the ages of 10 to15 years) during which the reproductive organs grow to adult size and become functional. The secondary sexual characteristics are termed ‘secondary’ because they develop after the primary sexual characteristics, which distinguish females from males.
Name some of the primary sexual characteristics of females.
You already learned about them in Study Session 3 — they are the anatomical structures of the external female genitalia (e.g. the labia minora and clitoris), and the internal female reproductive organs (e.g. the ovaries, uterus and vagina).
Menstruation continues every month, except during pregnancy, until the woman reaches the menopause at around the age of 48 to 50 years, when menstruation ceases. You may recall from Study Session 3 that at birth a female baby’s ovaries already contain about 60,000 immature eggs, and she cannot produce any more in her lifetime. By the time she reaches the menopause, her ability to bring ova to maturity has come to an end.
In Study Session 5, we describe what happens when an ovum is fertilised and it implants in the uterus and develops into a fetus.
Summary of Study Session 4
In Study Session 4, you have learned that:
- The hormones controlling the female reproductive system include gonadotropin-releasing hormone (GnRH), follicle-stimulating hormone (FSH) and leutenizing hormone (LH), all of which are produced in the brain; oestrogen and progesterone produced by the ovaries and the corpus luteum; and human chorionic gonadotropin (HCG), produced by the placenta during pregnancy.
- The menstrual cycle typically lasts 28 days, but it can be highly variable. It is characterised by menstruation from days 1 to 5 and ovulation at around day 14, but the date of ovulation is difficult to predict accurately.
- Menstruation is the monthly shedding from the uterus of the endometrium with some blood, which emerges through the vagina, typically for a period of three to five days. Menstruation continues from menarche to the menopause, except during pregnancy. It may also be suppressed by breastfeeding.
- The ovarian cycle refers to the regular, repeating events occurring in the ovaries during the menstrual cycle, characterised by the development of a few ovarian follicles; the maturation and release (ovulation) of a single ovum; and the formation and subsequent degeneration of the corpus luteum if pregnancy does not occur.
- The uterine cycle refers to the regular, repeating events occurring in the uterus during the menstrual cycle, characterised by the thickening of the endometrium and an increase in its blood supply, followed by its degeneration and shedding as the menstrual flow if pregnancy does not occur.
- The menarche and the development of secondary sexual characteristics signal the period known as puberty, when the internal reproductive organs grow to adult size and a girl becomes fertile and capable of becoming pregnant.
Self-Assessment Questions (SAQs) for Study Session 4
Now that you have completed this study session, you can assess how well you have achieved its Learning Outcomes by answering these questions. Write your answers in your Study Diary and discuss them with your Tutor at the next Study Support Meeting. You can check your answers with the Notes on the Self-Assessment Questions at the end of this Module.
SAQ 4.1 (tests Learning Outcomes 4.1 and 4.2)
The left-hand column of Table 4.1 gives the names of the various phases in the menstrual cycle. Complete the right-hand column by entering the correct period in days measured from the last normal menstrual period (LNMP).
| Phase of the menstrual cycle | Days (1 = first day of the LNMP) |
|---|---|
| Follicular phase of the ovarian cycle | |
| Luteal phase of the ovarian cycle | |
| Menstrual phase of the uterine cycle | |
| Proliferative phase of the uterine cycle | |
| Secretory phase of the uterine cycle |
Answer
| Phase of the menstrual cycle | Days (1 = first day of the LNMP) |
|---|---|
| Follicular phase of the ovarian cycle | 1-14 |
| Luteal phase of the ovarian cycle | 15-28 |
| Menstrual phase of the uterine cycle | 1-5 |
| Proliferative phase of the uterine cycle | 6-14 |
| Secretory phase of the uterine cycle | 15-28 |
SAQ 4.2 (tests Learning Outcome 4.2)
Why do you think that a woman may feel cramping pains in her abdomen when she is menstruating?
Answer
A woman may feel cramping pains in her abdomen when she is menstruating because the muscular walls of the uterus (the myometrium) contract to help cut off the blood supply to the endometrium, causing it to break away from the uterus.
SAQ 4.3 (tests Learning Outcome 4.3)
Can you suggest how the relatively high concentration of artificially produced oestrogen and progesterone in contraceptive pills prevents pregnancy in women who take the pills regularly as prescribed?
Answer
The relatively high concentration of artificially produced oestrogen and progesterone in contraceptive pills prevents pregnancy by activating a negative feedback mechanism on the hypothalamus in the brain. High levels of oestrogen and progesterone mimic the situation that occurs in pregnancy. They suppress the production of gonadotropin-releasing hormone (GnRH) from the hypothalamus, so the pituitary gland stops producing FSH and LH. This in turn stops the ovaries from maturing any more ova, so ovulation does not occur, and the woman cannot get pregnant as long as she takes the contraceptive pills regularly as prescribed.
SAQ 4.4 (tests Learning Outcome 4.3)
Explain why menstruation stops during pregnancy.
Answer
In a pregnant woman, the placenta continuously produces the hormone HCG, which causes the corpus luteum in the ovary to produce progesterone throughout the pregnancy. Progesterone maintains the endometrium as a thick fatty layer, so menstruation ceases during pregnancy because the endometrium remains attached to the uterus, where it assists in nourishing and protecting the growing fetus.